Archive for June 2007
A new weapon in the race for better drugs
This is an interesting article about a new class of biotechnology startups that are using new combination techniques and specialized ICT solutions to identify new drugs out of old ones.
Can an antipsychotic drug from the 1950s be paired with a 1980s antibiotic to shrink 21st-century tumors? Might an anticlotting drug help a steroid relieve arthritis? How about a cholesterol treatment and a pain reliever teaming up to tame diabetes?
Thought for the weekend
“A human being is born into this world fully equipped not only to take care of him or herself, but also to contribute to enlarging the well being of the world as a whole. Some get the chance to explore their potential to some degree, but many others never get any opportunity, during their lifetime, to unwrap the wonderful gift they were born with. They die unexplored and the world remains deprived of their creativity, and their contribution.” Full speech.
– Muhammad Yunus
Changemakers Global Health Competition – July 18th Deadline!
This is a fantastic competition that is being co-sponsored by Changemakers and the Robert Wood Johnson Foundation (RWJF). There is an initial award available for $5000 to anyone anywhere in the world and another $5 million up for grabs if you are a US based organization.
Please send this on to your networks.
Disruptive Innovations in Health
Changemakers is looking for entrepreneurs both within and outside of the health care field with ideas for new products, services, technologies, business models that enable consumers to manage health and receive care in ways that are more affordable, accessible, simple and convenient.
The unique competition model attracts solutions from social entrepreneurs from around the globe. Innovators submit their ideas and the Changemakers online community provides feedback on the problem and proposed solutions throughout the competition. This interactive process is designed not only to catalyze action on important issues but also to connect participants’ solutions with key decision-makers, investors, and health and social service providers.
Changemakers global network will select three winners from anywhere in the world—each of whom will receive a $5,000 cash prize. In addition, RWJF’s Pioneer Portfolio will review competition entries and may award up to $5 million to support projects (restricted to U.S. organizations) that show potential to go to scale.
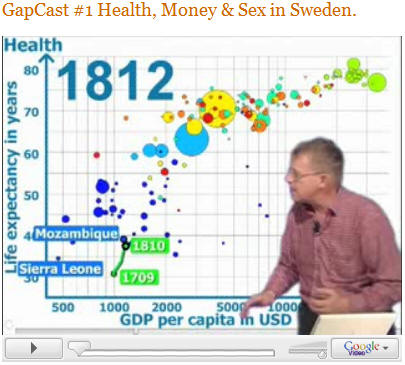
GapCast Debut: More Hans Rosling videos!
Hans Rosling has developed his first GapCast video with more on the way. This has me salivating after watching his TED speech using Gapminder software he helped develop and which was recently bought by Google (for related info to this, see our previous post on Google). Many people have seen the TED video, if you have not seen it, it is an absolute must watch (first video below). For those of you who have seen it, see him debut a new series with GapCast #1 – which is not as dramatic as the TED speech, but does demonstrate the power of his delivery and the software. We need more people to think like Hans – how can we get our message across in a different format, in a format that excites people, in a format they will not forget. The TED video is 20 minutes long, but it is worth it. Really great stuff:
Blogroll update…Global Health Journalism
I would like to note the addition of two fantastic blogs to our blogroll. The first, is SmallShift – “a blog built around the belief that technology in the hands of passionate users can inspire change…”
The second is Global Health Report, by the prolific science and medical writer – Christine Gorman. She will be a Nieman Foundation Fellow at Harvard where she will focus on global health media issues. Christine Gorman has written on health and medical topics for over two decades and has been at TIME Magazine since the mid 1980s where she had an award winning column (“Your Health”). In addition to her numerous other awards she wrote the 1996 TIME person of the year issue on AIDS expert David Ho. It is great to get a couple more outstanding voices in the lonely global health blogosphere.
On that note, I highly recommend reading Gorman’s speech at the Global Health Council on getting more involved and global health journalism. You can view her speech on her blog and see other coverage at Forum One. Enjoy!
Improved patient drug compliance using SMS
This idea has been mentioned a lot, but I just ran across Computainer on a Uganda listserv. CompuTainer recently announced SIMmed at the 3rd South African AIDS Conference. The technology uses SMS and USSD messaging to track and monitor patient compliance in taking chronic medication such as TB medication, ARV medication, Diabetic medication, Cardio medication and other chronic medication.
With 47% of patients simply forgetting to take medication and a further 33% not taking medication because they feel well we find an issue in medication compliance. With the ongoing struggle against drug resistant strains the introduction of SIMmed has resolved compliance issues.
I don’t have a copy of the report, but according to the listserv posting, in a recently completed trial in TB clinics in South Africa the compliance ratios were raised from between 20% and 60% to a staggering 85% to 93%. Cure rates were raised from a dismal 65% to above 91%.
The info on the SIMpill is copied here:
A pill bottle which, when opened, delivers an SMS text message to a central server. The SMS contains a unique pill box ID number as well as some information about the battery status of the pill box. Each SMS is time stamped. The central server receives the incoming SMS and, if it is within the time tolerances set for the pill box sending the message is simply stored for statistical purposes.
Low-cost zero emission lighting
Following up an earlier post on solar flashlights, I wanted to post this piece on a couple of light and solar devices in development. Check out the d.light forever-bright and Solar-in-a-Box system covered in the Launch Silicon Valley press release. Working from Mbarara now with intermittent power in the evening, the need for alternative power and lighting is, ah, blindingly obvious.
Sam Goldman and Ned Tozun, both second-year Stanford MBAs and co-founders of startup D. Light Design, want to eliminate the use of kerosene lanterns in developing countries with a product called Forever-Bright. The product’s working prototype is a white box about half the size of a loaf of bread with bright LEDs for interior home lighting and hookups to charge cell phones and power radios. The device can be charged with solar photovoltaic cells, or, for villagers capable of traveling to grid-connected power sources, they can charge the device and bring it back to their homes…
Installing residential solar power systems is too expensive, says Meredith McClintock, CEO of Petaluma-based ReadySolar, and her small startup wants to change that. Solar power, installed, currently costs around $10/watt. Approximately half of that expense is related to the cost of professional installation, says McClintock.
ReadySolar believes it can eliminate 30 to 50 percent of the installed cost with its Solar-in-a-Box systems, which come prepackaged and, the company claims, install more easily and cheaply than competing systems from big photovoltaic (PV)
installers such as Akeena Systems or Solar City.
Pharma Update: A Nuanced Approach to Drug R&D
Contribution by Dweep Chanana
Two interesting articles point to the future direction in the pharmaceutical industry:
BusinessWeek writes about Big pharma’s addiction for lifestyle drugs:
Try as they might to distance themselves from the lifestyle drug sector, pharmaceutical companies can’t seem to kick their addiction to these lucrative products. Even as consumers and government regulators grow more alarmed over drug safety, an examination of four popular lifestyle categories—weight loss, hair loss, sleep, and sexual dysfunction—shows that the pharmaceutical industry is by no means shying away from this controversial territory.
The Economist’s analysis of drug patents under attack in the developing world (from Thailand, to India and Brazil) is particularly illuminating:
At first sight, this row reflects an old dilemma that pits today’s patients against tomorrow’s. Compulsory licensing means that more Thais will get HIV drugs now, but it also means that drugs firms will be less keen to invest in drugs for Thailand in the future. Yet look closer and this is more than a fight between the poor-country sick and rich-world drugs companies. What makes it different is the role of two new actors: muscular middle-income countries and the rising generics industry.
What does this mean for drug development? Big pharma’s “truly innovative” drugs are being squeezed, and they can no longer count on a safe regulatory environment. And simultaneously, “lifestyle drugs” offer ample reward. Will innovation suffer – even more?
Beyond bringing to the surface that rhetorical question, the Economist does pose a useful question. The war on patents in the developing world is probably a good thing, as it pushes the envelope on what is legally possible under the Doha agreement – an agreement that has not yet been tested in international courts.
But it does create a problem. Countries such as India, Brazil and Thailand can indeed get cheaper access to certain drugs by issuing compulsory licenses. But the really poor countries cannot do the same as easily – not because they do not have local drug industries, but because they cannot resist pressure from the EU and US as effectively. As the Economist says, “a perverse result of this trend is that middle-income countries are getting cheaper drugs, whereas quieter and perhaps more deserving neighbours are not.”
It also shows how India’s own response to high drug costs will have to be more nuanced in future. India’s generics drug industry benefits from compulsory licensing. But its “R&D intensive” segment of the pharma industry – which includes Dr. Reddy’s and Ranbaxy – suffer. It was that segment that was most euphoric in embracing new TRIPS legislations. Expect them to lobby for stronger – not weaker – patent legislation. At the cost of India’s poor
Citizen journalism: outside a hospital’s doors
A slight digression here – here is a picture and commentary from the Virtual China, Institute for the Future, blog. I like the citizen journalism aspect that is (almost) real time raw imagery and associated opinions. Others have discussed the power of such techniques (check Yelvington, Huffington’s new effort, and ABC News cit journal new site) .
“Late night, June 12 2007, over 100 parents of sick children, and some children themselves, sleep on the ground in the underground parking garage and on the disabled ramp outside the doors of Beijing Children’s Hospital. In order to save the 20 RMB nightly cost of staying at the hospital…” Read the rest at Virtual China.

Donating money – as good as sex
A very small study found that charity activated pleasure centers in the brain. If this study is truly replicable and generalizable to a larger population then three things on the surface come to my mind:
1) Charities have a done a terrible job at recruiting people given that it feels great
2) It would be interesting to see the study substitute giving time for giving money
3) This holds promise for tapping into a human beings “pure altruism”.
If the same neurological areas are activated for doing good as for sex, pleasure and food, then you might think it could be easy to get more participation in charity events and more donations. Perhaps there is a need for better or sexier marketing and for other tactics. In the end there is not much new here, for those heavily involved in charity work and donating, you know it feels great and fulfilling, but this research can help create interesting advertisements or marketing campaigns (e.g. we could make the following t-shirts – Feel Sexy: Give Back) . Any thoughts on the t-shirts? Full Story:
“CHICAGO (Reuters) – Knowing your money is going to a good cause can activate some of the same pleasure centers in your brain as food and sex, U.S. researchers said on Thursday.
People who participated in a study got a charge knowing that their money went to a charity — even when the contribution was mandatory, like a tax. They felt even better when they voluntarily made a donation, researchers found.
“What is interesting is that these pleasure areas are for really basic needs, like food, sex, sweets, shelter and social connection,” Ulrich said in a telephone interview. “It’s the area that tells the brain what is good for us.”
DIY Beer Bottle Solar Water Heating
“Take 66 beer bottles. Fill them with water and connect so that it flows slowly from bottle to bottle. Place apparatus on roof (or better yet, build it in place) and voila, you have the ultimate in DIY solar thermal hot water systems.” Via Make Blog.

Solar power and Mbarara update

This is the second of two posts from UC Berkeley doctoral student Melissa Ho. Melissa is working on the Blum Center’s initiatives in six African countries. She’s got a few posts about the OBA work and I’m cross posting them.
Solar power and Mbarara update:
It’s been a busy couple of weeks, with not nearly enough access to internet cafes!
This week I am back in Mbarara, currently using the computer science lab (which is empty because the students are all doing exams now), but also meeting with various professors here (again!) and working with Ben and Richard on the Smartphones for OBA project.
The major update is that we are now collaborating with the Faculty of Science at Mbarara (Physics Dept) to figure out solar power options for the health clinics participating in the OBA program. They are currently engaged in research evaluating the degradation of imported solar panels and are the perfect collaborators for this project. They also have experience with circuit-soldering, so they’ll try to use Manuel’s solar charge controllers both for their own experiments and our project.
We also visited the Marie Stopes International Uganda office and one of the Marie Stopes Uganda clinics. They are currently using the VMUS database developed by Microcare, and have two people entering the data from the (triplicate-carbon-copy) forms that are collected from the various clinics participating in the OBA program. Right now the system is down, so the forms are piling up, and they are entering the data into Excel, so they can process the reimbursements. I’ll head back there today or tomorrow to hammer on the SmartForm and figure out exactly what it should look like. At the clinic we spoke to Steven about his experience participating in the program. The major issues he identified are timeliness of reimbursement processing, limitations on the range of treatment options (if someone is diagnosed with a non-STI bacterial infection then they have to pay for treatment in addition to what they paid for the voucher, although I think the consult is covered), and patients coming in with vouchers that clearly don’t have an STI, and therefore are not eligible for subsidized treatment. So there is a need for better and clearer marketing. Richard suggested giving distributors placards that (literate) patients can read so they know what services the voucher will cover. They also have problems with people going to multiple centers, and not having documentation for previous visits, or buying multiple vouchers and having tests done unnecessarily. We hope that with the SmartForms project we’ll be able to address some of these issues, by making voucher records more accessible, and improving the communications process around the form submissions. There’s lots of ideas flying around and a lot of work to do!
For the rest of the week (before I take off for Ghana) Richard and Ben and I will be visiting the various health clinics and talking to them about the project, getting a feel for their willingness/interest, as well as the environment in which the phones would be deployed. We’ll start testing/piloting in August when I get back.
Smart Delivery with SmartVouchers
I am back in Uganda until January working on the output-based aid project for STI treatment. There are several Berkeley projects in the country with some collaboration across project sites. TIER doctoral student and good friend Melissa Ho is working on the Blum Center’s initiatives across Africa this summer. She’s got a few posts about the OBA work and I’m cross posting them here.
Smart Delivery with SmartVouchers:
I’ve been in Uganda for almost a week now, doing a needs assessment with the East Africa Blum Fellows smartphone team – on whether and how smartphones can be used in the context of healthcare in Uganda. We’ve had meetings all over Kampala, with Satellife/Healthnet Uganda, the Ministry of Health, and various people at Makarere University. See my flickr account for a photo diary.
My most productive meeting so far has been with Francis and Gerry at Microcare, Uganda’s largest insurance company. Ben Bellows has been working with Microcare and Marie Stopes International on Output Based Aid (OBA), a voucher-based scheme for the delivery of STI treatment in the Mbarara district 6 hours drive west of Kampala (by the way, I just arrived in Mbarara yesterday). Ben and I (along with Mahad and Sonesh) have been talking about how to integrate smartphones into the voucher claims process and recently won a CITRIS award to fund the implementation of a pilot deployment. So when I arrived in Kampala, I made plans to meet Microcare and MSI to talk about our plans.
What strikes me most about Gerry and Francis is how fast they think. Having learned all about their insurance system, I asked why they didn’t use smart cards for the OBA program as well. In a flurry of conversation we realized that the smart cards are durable enough to be reused – and would be a useful platform for a new rural program promoting antenatal care. Rather than using vouchers, which could be resold or appropriated, they will issue smart cards for the 9-month duration of the pregnancy, recording visits. The “admission” into the program would be the cost of the smart card (about $1), and upon completion the patients would return the card in exchange for a small gift (we were thinking of baby socks). Within five minutes of my question, we not only had a whole scheme worked out, we also had a name: Smart Delivery. Using smartphones enabled with smart card readers we can set up a rural terminal such that transactions can be delivered efficently via SMS at extremely low cost. Within one hour, we had defined a protocol, and Francis had assigned the project to one of his software engineers (Microcare insources their work to a wholly owned software company in Chennai) and made plans to complete the work by June 15th. I’ll keep you posted on what happens! In the meantime, I’ve loaned them my two GPRS modems, so they will be testing the system using two PCs. I’ll see what I can do to implement the smartphone version…although it’s been entertaining trying to figure out the APIs without access to the web for documentation!
Capitalizing on the Mobile Revolution for Health Information Collection
Mobile devices and wireless connectivity options have advanced a swift pace. Many health care realize the potential of these mobile technologies to improve the accuracy, speed and efficiency of certain aspects of the health care infrastructure. The lowest hanging fruit in this regard is transferring paper-based reporting systems to digital media of one kind of another. The Stop AIDS project has developed wireless app to speed the processing of behavioral risk assessment surveys called WiFi Palm Surveys. It is not clear which Palm device they are using and why they have chosen that particular platform, but it seems that the forms are created using technologies from Anywhere Mobile Solutions based in Tulsa, OK. One big key to the sustainability of such efforts is the availability of cheap and reliable wireless connectivity. Luckily for Stop AIDS, San Francisco is in the midst of a large scale Wifi project. Click here for more info on the San Francisco Municipal Wifi project.
GlobalGiving “Sundance” Filmfest
This is a great idea. Check it out – “Here is how it works. We ask project leaders in the field to provide raw video footage, photos, and anything else they want to send in. Then we allow people to take that footage to create a video… In June, once all the films are submitted, we will launch public voting for the best videos.” Via Dennis Whittle’s blog. As of May 24th they were up to 290 film producers!!
(1) Click play below AND then
(2) Guide your mouse over the bottom of the screen to see 11 videos within the same screen – very cool stuff!).

SocialEnterprise TV
As I mentioned previously, video is really taking off. I have not had time to do a quality check of this latest venture [socialenterprise.tv] but do check it out and let me know what you think (also note the .TV extension, I had first seen that with Fora.tv):

“Coming soon… Internet TV for all things Social enterprise …. This channel is aimed at providing the Social Enterprise sector and its networks with a sector specific Internet TV channel, which is solely dedicated to promoting the work and strengths of social enterprise in an International marketplace… ”
And in case you missed it below, 3Four50 does have their own”channel” or set of show case videos that people can share:
![]()
Other video related websites I have covered in the past:
–Scribe
–KarmaTube (partnering with the Global Giving Film Fest)
–Fora.tv
–IET.tv
–Global Health TV
3FOUR50 – Collaborating Online against Chronic Disease
Ever gone to a conference and wished you could continue the work and discussions sparked there? The Oxford Health Alliance (OxHA) has come up with an online site, 3FOUR50, to encourage ongoing collaborations on chronic disease prevention.
![]()
The name 3FOUR50 comes from the combination of:
3 Risk Factors: tobacco use, physical inactivity and poor diet.
that lead to FOUR Chronic Diseases: cardiovascular disease, diabetes,chronic lung diseases and some cancers.
which cause over 50% of worldwide mortality.
As the fight against infectious disease progresses, we are in the midst of an epidemiological transition. Shortly, causes of mortality in the developing world will begin to mirror the mortality profile of developed nations – infectious disease mortality will drop, and the majority of mortality will be due to chronic disease.
3FOUR50 was conceptualized as an ‘open space for health’, to harness the social networking power of the internet to promote chronic disease prevention. All content is user-generated, and includes stories, blogs and vlogs (reflecting different cultural perspectives on health and comments/ideas from those wishing to share their views), high-profile guest interviews, photos, and full video coverage of the OxHA 2006 Annual Summit. 3FOUR50 was created by Tommy Hutchinson, Equator Media and Eddie McCaffrey of Joose TV, as a way of reaching a wider audience beyond the annual OxHA conference.
The mission of 3FOUR50, according to Eddie McCaffrey, is “to create an online space where anyone and everyone who has something to offer in the fight against chronic disease can come together to connect, collaborate and contribute. The space itself is about participation. We encourage a two-way (or even multi-way!) conversation, unlike many typical websites that simply offer users information without the ability to have their say.” He continues, “The success of the site will be measured by reaching a critical mass of people all over the world: researchers, health workers, academics, young people, business CEO’s, NGO’s, designers, whoever, wherever – who will exchange and share ideas, plans and projects with each other.”
The site concept was inspired by the idea of tapping into audiences that could not attend the OxHA conference and the ‘huge explosion in domains like myspace, youtube’ says Hutchinson. ‘Because we work so closely with young people, we see a lot of young people engaged in all of this.. up to now [these tools] haven’t been effectively applied in a social sphere. That really is our inspiration – [to take] some of the tools, techniques, the psychology behind a lot of this and apply it to a social sphere, and health is an extremely interesting area. How big [will it be?], we don’t think in terms of numbers, no one ever has any idea of how large, how far these things will go. Let’s just enjoy it and hope it makes a difference.’
The website was just relaunched with a new design and improved tools for collaboration:
Searchable new additions include:
A network page, where people can upload information about themselves.
Private collaboration space, where you can invite people to work jointly on a project (using Basecamp software)– has proved to be very popular in testing.
A ‘Soapbox’ channel, where you can upload information on your work with chronic disease prevention and share best practices with others, and get comments from around the world.
6 Billion Others: 6000 Interviews, 65 countries
I am a big fan of the photography by Yann Arthus-Bertrand, his latest project is related to his foundation for sustainable development. I will let the words below speak for themselves:
The Motivation:
“LIVING TOGETHER…We’re living in an incredible time…Over the past 50 years, mankind has modified the planet quicker and more extensively than in any comparable period of time in human history…and the sheer bulk of information out there has never been so huge…but what’s ironic is that in reality we know so little about our actual neighbors…in all the strife we’ve got coming to us, whether it’s because of poverty or climate change, we can’t do anything alone. The time when all you had to do was think of yourself is past and gone. From here on in you could say we have a duty to take care of each other…And the one way we can do that is to share life, talk to each other, stop being scared. There are over 6 billion of us and there is no chance of any kind of sustainable development if we can’t manage to live together. “

The Interviews:
“After the interviews a lot of people swore that what they’d told us they’d never said to another living soul…Every single person has got something interesting to say. And every single person has the right to say it, even if they don’t know it…I’ve been accused of exaggerating the feel-good side. That’s OK, there’s no shame in that. Goodness is a fundamental quality, and I have a lot of respect for it. “
Pricing Products for Developing Regions
The following research out of the Chicago Business School is worth a quick skim, or if you want a better digest, check out Foreign Policy’s view on this. Many of you will be familiar with this line of thinking, but it is not yet widely discussed in public health circles (as far as I can tell). As we know the bottom line is that giving something away for free is not always an optimal solution – economics/pricing, creating markets, and branding (along with a multitude of other factors) all impact behavior and use of products no matter where you go in the world. In our own research with Aurolab, we were told that when they actually tried to price their synthetic lenses for cataract surgery at a lower price people started questioning the quality (even though these two things were unrelated). I have some questions about extending the Chicago research on water purification products (time frame, sustainability, etc.), but it is good to see more work in this arena: