Archive for the ‘Innovation’ Category
Mosquirix – Promising New Vaccine for Global Health?
More than 12 years (let that time horizon sink in) after the first indications of success, there will be a large scale trial for a new malaria vaccine. The potential global health implications of this are obvious, read the full news article, it has some good tidbits in it:
“With the exception of Mosquirix, there’s no possibility of one coming on the market within five or six years…It took eight more years of development and testing before scientists were ready to conduct a large-scale trial of the vaccine. London-based Glaxo and its partners will begin a $100 million study of Mosquirix later this year, vaccinating 16,000 children in seven African countries. If the results are positive, the drug could be on the market as soon as 2011, making it the first vaccine against the deadly disease. “
Full article at Bloomberg (here). Hat tip to Families USA.
Global Health Video Makes Top 10 TED List
Everyone I have spoken to loves TED videos. If you aren’t familiar with TED, you are missing out. The Technology Entertainment and Design (there is that word again! see Jaspal’s work in the area of global health design) outfit gathers some of the best people in their respective fields to share ideas . While their annual conference is extremely exclusive, they do post their videos online. The tag line: Inspired talks by the world’s greatest thinkers and doers. TED just posted on the their top 10 videos in the past 2 years. On first glance I found 2 things remarkable about this list:
1. These videos have over 50 Million views (amazing)!
2. There is a global/public health video in the top 10, debuting at number 7
The numbers clearly display a strong appetite for for this kind of work – work that is innovative, connects and sometimes has great impact on the social good. What’s more – global health issues can garner a lot of attention and people do care about it (translation, there are ways to make it sexy and appealing). I would be very curious to get a age based demographic breakdown of who is watching these videos, specifically I want to see if there is a generational breakdown. The public health video has made its rounds and we did discuss it here at THD (I have posted it below again). From TED:
Announcing the Top 10 TEDTalks
“With 50 million views since we started posting video two years ago, TEDTalks have become a powerful cultural force. To celebrate this milestone, we’re releasing a never-before-seen list: the Top 10 TEDTalks of all time, as of June 2008.
With speakers like neuroanatomist Jill Bolte Taylor and global health expert Hans Rosling, the list proves one of the compelling ideas behind TEDTalks: that an unknown speaker with a powerful idea can reach — and move — a global audience through the power of quality web video…”
Hans Rosling (well worth watching):
Market Failure and the Clear Need for Electronic Health Records
The New York Times reports that Most Doctors Aren’t Using Electronic Health Records. However, the New England Journal of Medicine study released June 18th notes paradoxically “doctors who use electronic health records say overwhelmingly that such records have helped improve the quality and timeliness of care.” The benefits are overwhelmingly positive: “82% [of doctors using electronic medical records] said they improved the quality of clinical decisions, 86% said they helped in avoiding medication errors, and 85% said they improved the delivery of preventative care.” Clearly, electronic medical records could be a tremendous aid in improving health outcomes, shifting the balance of care from costly medical intervention to relatively inexpensive prevention measures, and reducing medical errors.
“Yet fewer than one in five of the nation’s doctors has started using such records.” Only 4% of doctors surveyed were using “fully functional” electronic records that can record clinical and demographic data, results of lab tests, issue orders and inform clinical decisions (such as warning about drug interactions). 13% of respondents reported using a “basic” clinical system, which lacks clinical decision support and some order-entry capability.
The barriers cited are largely economic, with doctors in small practices citing prohibitive capital costs for adopting a new system, lost income from not seeing patients, and no existing electronic medical record software that meets the needs of small to medium practices. In an attempt to speed adoption, the government has announced a Medicare program that will offer incentives to practices to transition to electronic medical records.
“What we see is a deficit in innovation, and that is something innovators and the capital markets can address,” said Dr. David J. Brailer, who leads a firm that invests in medical ventures, Health Evolution Partners.
After conducting several retrospective folder reviews, I believe the conventional patient folder is actually an obstacle to good patient care. Folders are often lost or duplicated, and they take time to retrieve. Basic patient information is duplicated in every physician’s notes, handwriting is often illegible, there is no alert system for medication errors, guidelines for patient management, or flags for unusual findings or reminders on lab results. Despite a fully integrated health system in South Africa, the reliance on paper records causes fragmentation of patient information, and disrupts continuity of care.
Why go with paper when you could have electronic medical records?
“Design Thinking” in Harvard Business Review (Tim Brown)
IDEO’s CEO, Tim Brown, wrote an article for June’s Harvard Business Review. This is a great introduction to design thinking.
If this link doesn’t work, go to the HBR website and look for the “Design Thinking” link. Currently it is accessible as free content.
Although many others became involved in the [Shimano “Coasting”] project when it reached the implementation phase, the application of design thinking in the earliest stages of innovation is what led to this complete solution. Indeed, the single thing one would have expected the design team to be responsible for—the look of the bikes—was intentionally deferred to later in the development process, when the team created a reference design to inspire the bike companies’ own design teams.
A couple extensions to Brown’s statements about the Aravind Eye Care System:
Much of its innovative energy has focused on bringing both preventive care and diagnostic screening to the countryside. Since 1990 Aravind has held “eye camps” in India’s rural areas, in an effort to register patients, administer eye exams, teach eye care, and identify people who may require surgery or advanced diagnostic services or who have conditions that warrant monitoring.
In developing its system of care, Aravind has consistently exhibited many characteristics of design thinking. It has used as a creative springboard two constraints: the poverty and remoteness of its clientele and its own lack of access to expensive solutions. For example, a pair of intraocular lenses made in the West costs $200, which severely limited the number of patients Aravind could help. Rather than try to persuade suppliers to change the way they did things, Aravind built its own solution: a manufacturing plant in the basement of one of its hospitals. It eventually discovered that it could use relatively inexpensive technology to produce lenses for $4 a pair.
First, Aravind did try to persuade suppliers to change the way they did things. The promise of a huge latent market was not convincing enough for existing suppliers to drop the price of their intraocular lenses (IOL). It was then that Aravind built its own capacity to produce lenses, in what came to be known as Aurolab. I would argue that both their attempts at negotiation with IOL manufacturers and their decision to produce their own lenses were reflective of design thinking.
Global Health Council 5: We ♥ Margaret Chan
Friday ended with an impressive lineup of global health leaders discussing the disconnect between horizontal and vertical funding in the plenary session titled Meeting Along the Diagonal: Where the First and Last Mile Connect. A webcast of this session, and 2-3 others from the Global Health Council Conference, will be available on kaisernetwork.org starting Tues-3-Jun-2008. It’s nearly 2 hours long, but brings together ideas from the Gates Foundation, WHO, the Global Health Council, and USAID. As much as it was about these organizations and the types of organizations (foundation, multilateral, advocacy, bilateral), it was about the individuals who spoke their minds:
- Jaime Sepulveda, Director, Integrated Health Solutions Development, Bill & Melinda Gates Foundation
- Margaret Chan, Director-General, World Health Organization
- Nils Daulaire, President and CEO, Global Health Council
- Henrietta H. Fore, Administrator, U.S. Agency for International Development, Director, U.S. United States Foreign Assistance
- Fore: “horizontal aspects to vertical programs”
- Sepulveda: “integration”
- Chan: “connect”
- Nils: “fractal”
- Stewardship
- Financing
- Delivery (personal and non-personal services)
- Resource Generation (people, information, vaccines, technology)
- Walsh J A & Warren K S. Selective primary health care: an interim strategy for disease control in developing countries. N. Engl. J. Med. 301.967-74, 1979.
- An “forgotten” article that Sepulveda wrote in the 1980s in the Bulletin of the WHO on the topic of “diagonalism”, but perhaps not in those words. (I wasn’t able to find it, but if you know of the article, please post a link as a comment.)
- Dentzer told her she was “the James Brown of global health”, a reference to her work ethic
- “What works for Hong Kong doesn’t work for Zambia.” This sounds obvious, but there was quite a lot of talk at this conference about exporting successful models from one country to another. I’m not saying you can’t learn from successes, but there is at least some better work we need to do in adapting those models to different situations.
- “Primary healthcare faded from the vocabulary of global health.” She cited Periago’s “crushed” comment from earlier in the day. In fact, she brought in a lot of examples of what other people were saying throughout the day, so it’s clear that she was listening.
- One of the other examples she brought up was a Johns Hopkins professor who in a morning comment advocated for “health impact assessments” like “environmental impact assessments” prior to doing something new. (Sorry, don’t know the name of the JHU professor.)
- “Famous soft drink”. She didn’t name it because she didn’t want to advertise for it, but asked “why can’t we get to the same areas of the world?” (a reference to technologies like vaccines and medicines). If we can’t do that, “we fail our people”.
- “It’s easy to blame people when you fail.”
- In referring to her 30+ years of experience: “I look young, but I’m not”.
- “Primary healthcare was alive” in places like Brazil, India, and Argentina, even though it wasn’t in the “official vocabulary”.
- “I’m not going to repeat the WHO definition of health. To me health is a social objective.”
- In indicating that we need to train more mid-level professionals: “For the clinicians in the audience, don’t worry, there’s plenty of work.”
- “We have not listened enough.” “We underestimate the ingenuity of the community.” “If you say ‘talk is one thing, walk is another’, I rest my case.”
- “We are insular. We only look at the health sector.” We need to look at safe water and sanitation, education, etc.
- “Ministry of Health [alone] cannot handle the complexity of the situation.”
- “Let’s be realistic. Even NGOs are making profits.”
- “Why is it that working with industry is seen as dirty?” “Industry is part of the solution.” We need to work with food and pharmaceutical industries.
- Peer review is “another elephant in the room”- Chan identified most of the elephants. It is a process by which “your friends condone your work”.
And my favorite, because it directly addresses the work I do and that we need to advocate for in the development of new technologies and services:
- “I didn’t realize that the color of bednets makes a difference.”
- “It wasn’t until we brought in the anthropologists that we found out that the color red represented death.”
- They changed the color to yellow and people started to use them.
Global Health Council 4: Coming Full Circle with Aravind
Aman already reported on the Aravind Eye Care System (AECS) being awarded the prestigious 2008 Gates Award for Global Health, which “honors extraordinary efforts to improve health in developing countries”. And as Aman mentioned, three of us at this blog owe a big debt to the Aravind organization, first for allowing us to work with them starting in 2004 in studying the Aurolab model, and second for launching us into the arena of technology, innovation, and global health. More than 4 years after we began our relationship with Aravind, I found myself at my poster talking with Dr. Nam and Dr. Ravi about medical licensing for recent graduates in India and Mongolia. (Similar policies of requiring graduates to work in rural areas between medical school and residency.)
The photo below is from after the awards ceremony on Thursday night. L-R: Dr. R.D. Ravindran, Chief Medical Officer of the Pondicherry hospital, Dr. P. Naperumalsamy, me. Thanks to Suzanne Gilbert, Director of the SEVA Foundation, Center for Innovation in Eye Care, for taking the photo. She was also instrumental in getting us started in this field, so it was great to reconnect with her here in DC.

Dr. Nam’s award acceptance speech on behalf of AECS followed up a short film about Aravind and a detailed telling of the Aravind story by William Gates, Sr. Some new directions I learned from his speech:
- Aravind has signed an MOU with China to increase the number of cataract surgeries done there
- They have an increased emphasis on information technology for supporting and extending services
- They aim to provide 1 million cataract surgeries per year within 5 years (currently 280,000)
- On October 1st, they will dedicate a research institute named after Dr. V
Dr. Nam closed by saying: “We have done something through Aravind, but there is much more to be done.”
Global Health Council 1: Social Marketing
On Tuesday of the conference, I attended the Social Marketing to Facilitate Behavior Change and Action workshop. I personally found it to be very educational, although I did have one gripe (see #3 below). A few thoughts I had during the workshop:
(1) Creating new products and the lead user. In describing the role of social marketing, the facilitators considered the question “how do we make the choice easier [for adopting healthier behaviors]?”. Their answer was “creating new products” and the example they gave was the LifeStraw. A woman from Vestergaard-Frandsen, the company that makes LifeStraw, was in the audience and shared the story of the conceptual development of the product – it seems this was a case of a lead user. One of the fieldworkers who worked on a national Guinea worm eradication campaign created her/his own life straw with reed and some mesh for local use.
(2) Social marketing and social design ethnography. The reason I went to this workshop was to establish a better understanding of how my work relates to social marketing. My work uses applied ethnography for the purposes of design in global health, not just products, but also services and systems. While there is considerable overlap, the idea of creating new products felt like an awkward fit within the framework of social marketing. I expect it was there because it has no other home (e.g. social product design). The danger in placing it in the context of social marketing is that it may ignore the considerable knowledge we have developed and are developing in the field of human-centered design. There is also a difference in the methods. Ethnographic research seems play a minor role in social marketing, and as in many fields, the label ethnographic seems to be used fairly loosely.
(3) Know your audience. The majority of examples (not all) in the workshop were drawn from the US context (e.g. commercial advertisements, surveys, anecdotes), and further weren’t well-contextualized. Not what I expected at a global health conference, with a very international group, where the focus of the workshop was “know your audience”.
(4) Adapt, don’t adopt. One of global health’s strengths is that it borrows from so many diverse fields. The dangers with this are in simply adopting the idea rather than adapting it to the contexts of global health. In the case of social marketing the ideas that have been borrowed are framework (effect behavior change), process (how to understand your consumer), and theory (behavior change models). The typical dangers of doing this are: (a) what is borrowed can be viewed as gospel (e.g. if Madison Ave. does it this way, it must be right) or (b) the ideas don’t progress as they do in the original field (e.g. is social marketing making use of advances in commercial marketing? is it evolving on its own?). I still don’t know enough about social marketing to argue this, but I’ve seen this pattern with other ideas that have been borrowed across fields.
(5) “We’ve already been doing this”. One of the audience members brought up the fact that people have been doing this for a long time in many places and that it simply hasn’t had the “social marketing” label. Agreed, but in my opinion – and that of the facilitators – the value is in the framework. By creating a formal way of thinking, we can improve the social marketing work that people have been doing by other names, and bring it to people who haven’t been thinking in these terms.
Ben was there for part of the workshop and may have more thoughts.
Update from Aman – here are some other great resources in the area of social marketing:
http://socialmarketing.blogs.com/
http://pulseandsignal.com/
http://www.social-marketing.com/blog/
Redesigning Technology for Global Health
 This is an interesting story — GE redesigning an EKG machine (the last one of which they made in 1999) for a place like India. The have also been advertising a lot on TV – I was able to find the ad on YouTube which is pretty cool. Four things immediately struck me:
This is an interesting story — GE redesigning an EKG machine (the last one of which they made in 1999) for a place like India. The have also been advertising a lot on TV – I was able to find the ad on YouTube which is pretty cool. Four things immediately struck me:
1) The accomplishment – Cost reduction from $10,000 to $1500 in under 2 years and weight from 15lbs to 3lbs!
2) The original machine took 3.5 years and $5.4 million to develop. Compared to drug development this is minuscule. Making devices is generally orders of magnitude cheaper, far quicker to develop and face far fewer regulatory hurdles (FDA). So why didn’t this happen sooner?
3) This is great for India, but what about for use in the US (especially for community clinics and in rural areas)?
4) Let’s not forget that the introduction of any “new” technology will have unintended social consequences which are sometimes horrendous, here is another example from GE and their ultrasound machine.
EKG Story:
“GE Healthcare engineer Davy Hwang’s marching orders were straightforward. Take a 15-lb. electrocardiograph machine that cost $5.4 million and took three and a half years to develop. Squeeze the same technology into a portable device that weighs less than three pounds and can be held with one hand. Oh, and develop it in 18 months for just 60% of its wholesale cost. ‘He thought I was crazy’…” Crazy or not, Hwang pulled it off…The result: The new MAC 400, GE’s first portable ECG designed in India for the fast-growing local market.”
Full story at Business Week.
Related Links:
NIH and India partner to develop low cost medical technologies, Link
Medical basics still needed in developing countries, Link
Innovation for Global Health Course
Jose from Little Devices That Could (LTDC) is going to be helping out with a fantastic looking course being offered by Harvard-MIT. The post below, with permission, is from LTDC. The course has some very bright minds involved. Could you imagine a collaborative course like this on every campus? I would bet there would be some great results. If you have any input or project ideas, send Jose an email (see his website below).
UPDATE: This course will be available via:
1. opencourseware
2. telecast (with hope of reaching overseas univs also)
3. open access to materials
4. potential roll out in other schools in 2009
From Little Devices that Could:
LTDC Goes to Graduate School: Harvard-MIT announce HST 939, Designing and Sustaining Technology Innovation for Global Health
Following a long history at MIT of incredible classes like D-Lab, Developmental Entrepreneurship and S-Lab from Sloan School of Management,the joint program in Health and Technology by Harvard and MIT have announced HST 939:Designing and Sustaining Technology Innovation for Global Health.
The class will focus on exploring new ways and avenues of answering global health’s most vexing problems at the intersection of business, public health, and disruptive technologies. Hands on participation in real life projects with international community and corporate partners will allow students to experience global health development 2.0 from the start.
The class is the brainchild of HST affiliate Jeff Blander, a social entrepreneur and global health expert, who teamed up with Utkan Demirci, a scientist and inventor at Harvard with a shared focus on global health technologies. They’ve asked Yours Truly to participate in the design and instruction of the technology and bottom-up innovation aspects of the class, and I’ve heartedly agreed.
If my posts have been infrequent lately, I apologize, but the there has been a lot of work to set up some exciting projects which I will be sharing with you shortly. We are continuing to receive a lot of interest from corporate and foundation sponsors about their own projects and the door is open for continuing collaboration. One of the most exciting aspects of the course is its commitment to cross-institutional collaboration. The current partners include companies, NGOs, and other academic institutions beyond Harvard and MIT. So get ready, in a few months, we’ll be highlighting the next little devices that could—and the business report cards that go along with them! Everything starts in Spring 2008, but you can submit your projects now!
World AIDS Day: Educational Breakthrough
Tomorrow is World AIDS Day and instead of “barraging you with [another set of] statistics, gruesome photos, or heart-wrenching stories” (quote credit to Mr. Casnocaha), I want to alert you to something we prefer here – solutions, problem solving, technology, and creative thinking. Piya Sorcar, a doctoral student in Stanford’s Learning, Sciences & Technology Design program has used her considerable skills to figure out how to reach the minds of children in devleoping countries when it comes to HIV/AIDS education.
Incorporating a variety of techniques from several disciplines Piya has generated an animation based educational technique and curriculum, the first of its kind in this area. The first results from this groundbreaking technique are in and they have been outstanding. The indefatigable Sorcar has plans to disseminate the educational curriculum free to schools and other organizations. She also has plans to launch the animation on social networking sites such as Orkut (very popular in some developing countries) and Facebook.
This educational technique and curriculum has taken over 2 years to develop and as far as we know no one else is using this animation based method. This work is truly inspirational, overcomes various methodological barriers and just as importantly political barriers (especailly in countries where sex education is banned). The early results indicate tremendous success. I highly encourage you to read the full story below and visit the website where the animation can be viewed: http://www.interactiveteachingaids.org/
We previously covered Piya Sorcar’s work in a post last year and it has been the most read post on this blog with over 1700 visits. You can view that here for further background information.
Lasly, there is much more to say about Piya’s work which we will save for another post. I have placed some links about World AIDS Day below this entry and as a side note – even rock group Queen is getting into the action with their first new recording in a decade to mark the event.
Enjoy!:
Doctoral student creates groundbreaking animation to teach HIV/AIDS prevention in developing countries
To combat the stigma associated with discussing HIV/AIDS and sexual practices in India and other developing countries, doctoral student Piya Sorcar has developed a groundbreaking animation-based curriculum to teach HIV/AIDS awareness and prevention in a culturally sensitive manner to young adults around the world.
Sorcar’s project, Interactive Teaching AIDS, is already being used in several countries…The animation emphasizes the biology of HIV/AIDS, presenting a storyline with a dialogue between a curious student and a friendly yet authoritative cartoon “doctor” on the biological facts about HIV,its spread, and its prevention.
“What’s groundbreaking is that she’s shown that we can inform people about AIDS while respecting the culture,” said Communications Prof. Clifford Nass, an advisor to Sorcar’s Ph.D. project. “That’s an enormous accomplishment.”
“The result was Interactive Teaching AIDS, an animation-based tutorial featuring a friendly cartoon doctor and patient who guide participants through the biological aspects of AIDS transmission. The tutorial is available online and on a CD.”
RESULTS
A recent study of the application in India by Sorcar with 423 students in private schools and colleges in North India, showed significant gains in learning and retention levels after interacting with the 20-minute animated tutorial. Prior to testing, only 65% knew that HIV was not spread through coughing; after the tutorial, this percentage increased to 94%. Students stated that they were comfortable learning from the tool, and more than 90% said they learned more about HIV/AIDS through the animated tutorial than any other communication method such as television or school. One month after initial exposure to the tutorial, students were rapidly seeking and educating others about HIV/AIDS prevention through their networks, with nearly 90% sharing information they learned from the tutorial with someone else.
Full story and above sources from here and here
More links:
CNN Student Learning Activity, link
MTV and KFF Partnership, link
NPR story, link
Reuters article, link
Beyond Good Intentions Documentary
Beyond Good Intentions:
What Really Works In International Aid?
“The Beyond Good Intentions film will document effective examples of international aid and inspirational humanitarians who are making the world a better place through their work. This is a rough cut trailer for the documentary film that is taking us around the world to ten different countries over the course of a year including Colombia, Peru, Argentina, India, Cambodia, Laos, Indonesia, Madagascar, Mozambique, and South Africa.” See trailer below, actual story profiles begin at the 3:15 minute mark (via Change the World blog):
Forbes on Fixing Healthcare in Africa
Its great to see a generally conservative business magazine discussing positive, successful global health efforts in Africa. Forbes has 3 very recent pieces that are worth skimming. Again, this is yet another indication of increasing convergence of the social and business sectors that we had previously profiled (trends in global health coverage by the business press).
The Rwanda Cure: Success Stories
Forbes Oct 29.2007, link
Western do-gooders are pouring billions of dollars into ontrolling malaria, AIDS and other killers ravaging the world’s poorest continent. Now comes the hard part…Some of what sub-Saharan Africa needs is new technology, like a malaria vaccine. But what’s needed most, particularly in Africa, is better logistics.
“The hardest truth for people to come to terms with is that the practical solutions are already out there, but they are not being applied…Donors always want to do something new. The simple things aren’t so glamorous.” Full story
In Pictures: Seven Ways To Fix Health Care In Africa
Follow this link
HealthStore to expand to Rwanda, link
How do you get basic care to the remotest villages in Africa? One clever idea is to borrow tactics from retail chains like McDonald’s and Subway–operate an easy-to-replicate, owner-operated franchise system focusing on health care.With a budget of under $1 million a year, HealthStore Foundation subsidizes nurses in rural areas to run 65 for-profit retail clinics in Kenya that provide basic treatments for malaria, respiratory infections and worms.
Nurses pay about $300 to buy a clinic, and sell medicines for a modest profit at a retail price of $1. The 65 clinics run under the name CFW Shops and treated 400,000 patients last year. Many are run by retired nurses lured back to work by the prospect of owning their own business.
Full story here.
Using Virtual Online Worlds to Research Epidemics
This is a fascinating idea that was sent to me by Cat Laine over at AIDG. I know I am always raving about their blog, but really if you haven’t managed to check it out – go over there right now. Onto the story which may or may not have benefits for modeling real world epidemics: “A fantasy plague that accidentally ran amok in the Internet’s most popular game world, populated by nine million flesh-and-blood players, may help scientists predict the impact of genuine epidemics…”
This story is not only a case of researchers being very innovative but also yet another example of how the business world is getting invovled and make a contribution to solving global health problems. The company that makes World of Warcraft is Vivendi a, giant global media company, that has entered into dicussions to possibly provide scientific data for research.
Online gamers rehearse real-world epidemics
“Virtual playgrounds such as World of Warcraft, launched in 2004, could soon become testing grounds for the all-too-real battle against bird flu, malaria or some as yet unknown killer virus….As technology and biology become more heavily integrated in daily life, this small step towards the interaction of virtual viruses and humans could become highly significant.
The unlikely path to a collaboration between hard science and hard-core gaming began in late 2005, when Blizzard programmers introduced a highly contagious disease — dubbed “Corrupted Blood” — into a newly created zone of the game’s Byzantine environment.
World of Warcraft is a “multiplayer online role-playing game” in which players — numbering in the tens, or hundreds of thousands — use computer-controlled avatars to fight battles, form alliances, and dialogue simultaneously on the Internet. At first the “patch”, as new elements such as the disease are called, worked as expected: experienced players shrugged it off like a bad cold, and weaker ones were left with disabled avatars.
But then things spun out of control. As in reality, some of those carrying the virus slipped back into the virtual world’s densely populated cities, rapidly infecting their defenseless inhabitants. The disease also spread — much like real influenza or the plague — via domesticated animals abandoned by players for fear of infecting their avatars, leaving the sickened pets to roam freely. Programmers tried to set up quarantines, but they were ignored. Finally, they resorted to an option not available in the real world: they shut down the servers and rebooted the system.
This was the first time that a virtual virus has infected a virtual human being in a manner resembling an actual epidemiological event…To date, epidemiologists have relied heavily on mathematical simulations to forecast the spread of contagious diseases across large populations.” But crunching numbers has limitations, says Fefferman. “There is no way to model how people will behave” in a pubic crisis, she said.
“How many will run away from a quarantine? Will they become more or less cooperative if they are scared? We simply don’t know.” Which is where the virtual netherworlds come into the picture. They can help scientists to “feed appropriate parameters into existing epidemiological models,” she said.
—
Other video game uses for public health:
1) The Wii (check out this review of the Wii for health, Nintendo’s Wii finds use in physical therapy)
Life Saving Design: Coke Can Syringe Disposal
I lifted this from our good friend Jose over at Little Devices that Could. It was part of the INDEX: Design to Improve Life competition (see People’s Choice Award 2007). Business Week has a full profile of this invention that you should see for clear pictures and a description of the safe locking mechanism. Also the comments section bring up some good questions about using a soda can for disposal. Check out the BW story: Life-Saving Design.
The Problem:
According to the WHO, some 16 billion injections are administered globally. In 2005, contaminated needles led to 260,000 HIV infections, 1.3 million early deaths, and 23 million cases of hepatitis. WHO researchers estimate that as many as 50% of injections in developing countries might be unsafe.
One Solution:
Antivirus, the simple design she came up with as a result of her childhood ordeal, just scooped the People’s Choice prize at the prestigious Index: Awards, touted by organizers as the world’s largest design prize…Antivirus is a lightweight plastic cap that fastens to any metal soft drink or beer can, which medics can use to remove and sequester dangerous syringes…The straightforward concept transforms a ubiquitous piece of trash into a potentially life-saving device. See more at Business Week.

TruDiagnosis: The Ultimate Diagnostic Device
Wired magazine has a fascinating piece from last month on the “ultimate medical diagnostic device” which is being developed in collaboration with the private sector. It is by Thomas Goetz who runs his own blog: Epidemix. Excerpts below:
“Our inability to diagnose and track infectious disease quickly and accurately remains a serious problem…The problem with cultures is that they take a long time — three weeks or more — to produce a definitive result. In those three weeks, antibiotics may be fortifying the bacteria’s resistance rather than curing the patient. In those three weeks, a TB patient goes back into the population and spreads disease. In those three weeks, the bacteria have enough time to escape our grasp. What’s needed, then, is a new way to diagnose the disease: one at least as fast as the sputum microscopy test, as accurate as the culture, and refined enough to differentiate between garden-variety bacteria and drug-resistant strains. What’s needed is nothing less than a new gold standard…Those tests might finally be at hand. There is a crop of diagnostic tools on the horizon… Dozens of companies are investing hundreds of millions of dollars to develop these new tools.”
“TruDiagnosis: It combines advances in microfluidics (miniaturized pumps and channels), microarrays (micron-sized sensors affixed to a chip), and engineering into what could be the ultimate medical gadget: a handheld device that, using a small sample of blood or spit, reveals in mere minutes every pathogen inside the body.”
From KaiserNetwork: “Researchers Use GPS, PDAs for Malaria Prevention in Africa, Study Says”
CDC researchers have developed new tools using GPS technology and PDAs to help prevent the spread of malaria in Africa, according to a study published in the August issue of the American Journal of Tropical Medicine and Hygiene, InformationWeek reports. Researchers used the devices to collect data on the use of insecticide-treated nets in homes in Niger and Togo.
The researchers used sampling software for Windows Mobile devices to compile complete lists of households in the area and employed GPS systems to locate homes and interview a random sample of people. Study co-author Jodi Vanden Eng in a statement said, “Before we developed this method using these devices, it usually took days, or even weeks to complete the same task” that the researchers now can accomplish in one day.
Full story summarized on KaiserNetwork.
Blood, Sweat Could Power New Paper Battery
 This technology is still in development and so I have no idea what the cost is going to be. However, without considering costs, this may have potential for use in low resource settings:
This technology is still in development and so I have no idea what the cost is going to be. However, without considering costs, this may have potential for use in low resource settings:
“Morning Edition, August 27, 2007 · Blood and sweat could power a battery that looks just like a piece of paper, scientists say…the new paper battery can run on blood or sweat. That means it might ultimately be used to power medical devices like hearing aids or pacemakers.” NPR full story.
Global Health Diplomacy: Rx for Peace
An interesting commentary piece in yesterday’s Washington Post, excerpts below:
Health diplomacy: Rx for peace
Susan J. Blumenthal/ Elise Schlissel
The Washington Times
August 26, 2007
“A survey of Americans’ political and social values reveals that belief in the effectiveness of military power as a foreign policy tool has dropped to the lowest point in the last 20 years…This diminished confidence in military intervention as a cornerstone of international relations raises an obvious question: What other tools are available to advance U.S. interests in the world? Health diplomacy is an important and underutilized instrument in our nation’s foreign-policy toolbox.”
“More than 63 percent of the people infected with HIV live in Africa; 79 percent of the chronic disease burden is in the developing world. Whether “over there” is Africa, Southeast Asia or Latin America, inhabitants of the United States for far too long have seen little reason to worry. But Americans — and the world — have much to gain from increasing our focus on global health.”
“Health diplomacy is a means of self-preservation in an increasingly interconnected global community. SARS, H5N1 avian influenza, AIDS, TB — the list goes on and on — are only a jet plane away from America’s shores. Globalization facilitates the rapid response to health problems between rich and poor nations by quick mobilization of health professionals, medicines and supplies, and deployment of information technology for surveillance of diseases and sharing health information and best practices worldwide…”
“The United States spent $571.6 billion on defense last year alone, but spends only 0.14 percent of its gross national product on global health and development, the least of any major industrialized nation…”
“For example, the tsunami relief efforts in Indonesia: A poll found after the visit of two former U.S. presidents coupled with a commitment to invest significant funds toward rebuilding communities, support for the United States rose from 36 percent to 60 percent virtually overnight in the world’s largest Muslim country, while support for Osama bin Laden dropped from 58 percent to 28 percent.” Full commentary here.
Tournistrip: Simple and cheap tech for reducing hospital infections
There will surely be challenges to adapting the “Tournistrip” to low resource settings, however, it is a cheap and simple way to cut hospital infections due to the high volume reuse of traditional tourniquets. I am just shocked that they don’t already do this in hospitals found in the West:
“Two recently qualified doctors believe they could have found an important weapon in the fight against hospital acquired infection – and it costs just pence.” Full story at BBC News: Simple band could cut hospital bugs.
Vinegar, cotton and light used to detect cervical cancer
In place of unaffordable pap smears, 8 years ago researchers at Johns Hopkins validated a “simple method” for detecting cervical cancer: the use of vinegar. That study was conducted in over 10,000 women across 15 clinics in Zimbabwe (1999 BBC news story). Fast forward to this month and we have a re-validation of this method in 50,000 women in India. A new study was conducted from 2000-2006 (hat tip to Drug Wonks):
A cheap method to detect cervical cancer using vinegar, cotton gauze and a bright light could save millions of women in the developing world, experts reported Friday. The study, published in The Lancet medical journal, found a simple visual screening test to look for the early signs of cervical cancer reduced the numbers of cases by 25%. “This is a landmark study,” said Dr. Harshad Sanghvi, medical director at JHPIEGO…Experts think that the simple, inexpensive technique could be rolled out across the developing world relatively easily. Pilot projects are already under way in a handful of countries in Asia and Africa. Full story: Simple Method Detects Cervical Cancer.
iPhone for Global Health
There is not much left to say about the iPhone, it is clearly one of the most hyped electronic gadgets in history and it is an understatement to say that it has lit up the internet (a google search for iPhone yields 103 million hits, compare that to only 70 million hits for a google search on “paris hilton”). It looks like an enterprising non profit decided to see if they can use the iPhone hype to market their cause (getting anti-retroviral treatment to children infected with AIDS in Africa, KCA website). They were first in line at a New York store in order to get an iPhone that they will auction off. The “first iPhone sold” will be presented by Alicia Keys at the Black Ball.
As the highly anticipated iPhone launch approaches, so does the promise of improved communications and connectivity with people around the world. Connectivity is not limited to technology; rather, it’s a fundamental fact that we are “one.” source… Supporters of Keep A Child Alive took advantage of the wildly hyped iPhone launch by standing in line for 4 days and communicating the charity’s grass- roots mission to New Yorkers and media from around the world. At 6 pm on Friday, June 29th, Spike Lee, renowned director, producer, writer and actor, joined Keep A Child Alive volunteers at Apple’s Soho location to purchase the first iPhone.” Full story, Earth Times
I would guess that getting in line on Tuesday will have garnered more knowledge and advertising about their cause than the auction will. I am not sure what the impact has been on the organization, but it is certainly a unique and innovative idea. They have been smart about getting the word out. Of course there is the publicity they received from actually being first in line, but in addition to that, I have seen their cause mentioned on widely popular techie websites such as InfoWorld, Gizmodo and Endgaget and on other sites they have partnerned with (iphonelaunch.tv). The Taproot Foundation also had someone in line for charity (see stories here and here). Some pics below from the folks at Keep a Child Alive (via flickr):

“This morning we started lining up for the iPhone – we are first in line at the Soho Store! We’re doing it with our friends at Keep A Child Alive an amazing organization that provides drugs for kids in Africa.”



Subscribe to this blog here
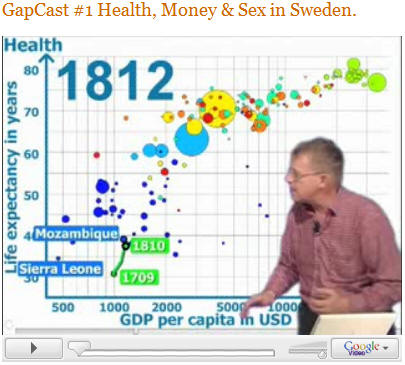
GapCast Debut: More Hans Rosling videos!
Hans Rosling has developed his first GapCast video with more on the way. This has me salivating after watching his TED speech using Gapminder software he helped develop and which was recently bought by Google (for related info to this, see our previous post on Google). Many people have seen the TED video, if you have not seen it, it is an absolute must watch (first video below). For those of you who have seen it, see him debut a new series with GapCast #1 – which is not as dramatic as the TED speech, but does demonstrate the power of his delivery and the software. We need more people to think like Hans – how can we get our message across in a different format, in a format that excites people, in a format they will not forget. The TED video is 20 minutes long, but it is worth it. Really great stuff:



You must be logged in to post a comment.